
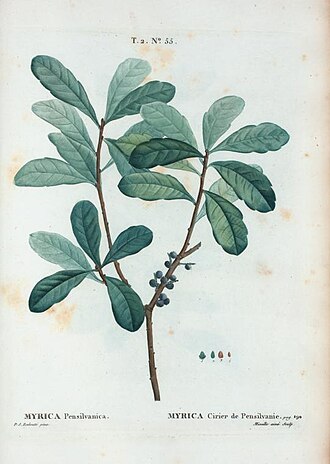
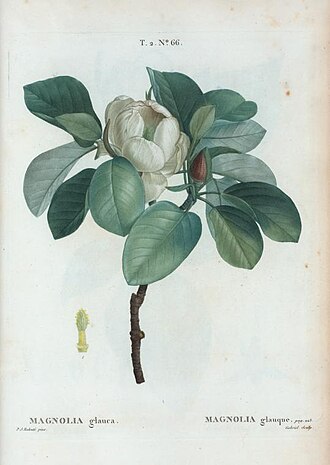

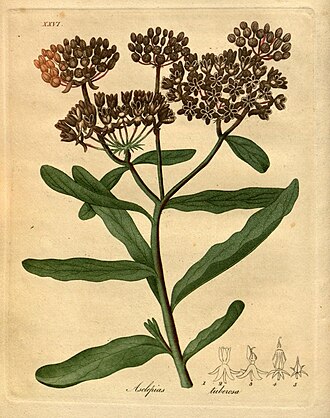


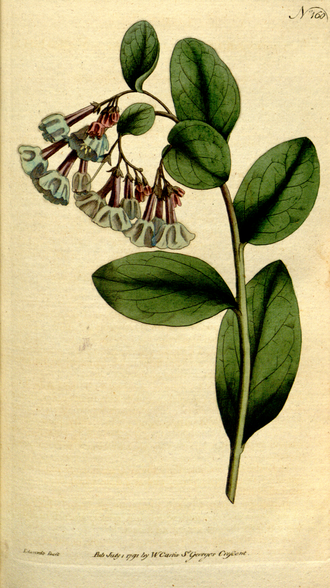
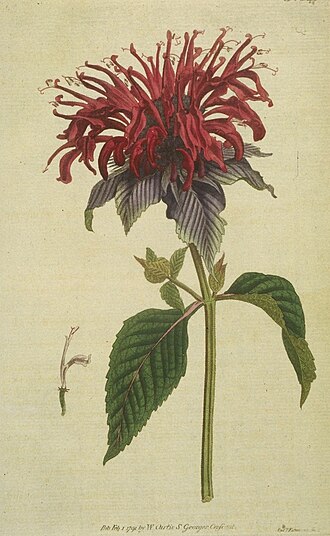
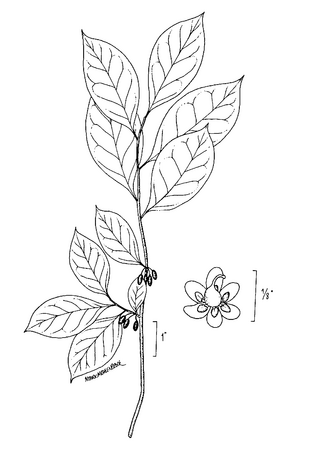
Native plants of Sussex County, DE · All illustrations public domain · Walcott (North American Wild Flowers, Smithsonian 1925); Redouté (Traité des arbres); Curtis / Edwards (Botanical Magazine, 1787–1804); Bigelow (American Medical Botany, 1818); Michaux (North American Sylva, 1819); Köhler (Medizinal-Pflanzen, 1887); Britton & Brown (Illustrated Flora, 1913); Sprague; Sepp (Flora Batava, 1814) · Wikimedia Commons · Mt. Cuba Center · Longwood Gardens · UD Extension · DE Inland Bays · DE Nature Society
For 1–2 years, something has been shifting in how my brain tracks where my body is in space. The medical word is proprioception — the inner sense of body position. When it's off, you don't feel dizzy. You misjudge distances and collide with things.
This pattern is new. I've had cochlear implants for years with no such problem. Something changed in the last 1–2 years — the implants are not the cause of the new onset.
When I'm cooking for guests or managing a lot of plans, the misjudging gets worse. This is not psychological — it has a specific neurological explanation called Dual-Task Interference.
Being deaf and using cochlear implants means my brain already works harder than most people's to interpret sound and orient in space. That raises my baseline load. Add hosting and planning — the system reaches its ceiling.


Nutritional deficiencies can cause fully treatable proprioceptive neuropathy. These should happen at the very first visit — cheap, fast, rules out a fixable cause before genetic testing begins.
Mother had dizzy spells. Son has dizzy spells. I misjudge distances and hit things — pain from contact, not dizziness. Three generations, different presentations of possibly the same gene.
This may explain why mother had "dizzy spells," son has "dizzy spells," and I experience proprioceptive pain on collision — the same underlying gene presenting differently across three generations.
Each child has a 50% chance of carrying the same variant. Genetic counseling is recommended for the family.

The research finding above applies here in an important way: even in patients who can have MRI, brain imaging rarely changes management for this presentation. The conditions that best fit — SCA 4, SCA 25, B12/copper neuropathy — are known for normal-appearing brain scans. NCV, SSEP, blood work, and genetic testing are the diagnostic tools that actually matter.
1. Paraneoplastic cerebellar degeneration (PCD)
2. Chemotherapy-induced peripheral neuropathy (CIPN) — taxanes
3. How to distinguish PCD vs. CIPN vs. hereditary SCA clinically
Medicare covers EMG/NCV when medically necessary. Medicare pays 80% of the approved amount; Medigap Plan G pays the remaining 20%. The Medicare-approved rate for a full sensory NCV study is roughly $150–$350 — your cost after Medigap is $0 (after the ~$257 annual Part B deductible is met).

Covered under Medicare Part B when ordered with appropriate clinical indication. Medicare-approved rate ~$100–$200; Medigap covers the 20% coinsurance.
CPT 92548 (computerized dynamic posturography). Medicare may cover under vestibular testing benefits — coverage depends on the clinical indication documented. Ask the ordering neurologist to submit prior authorization if needed. If not covered, many ataxia centers include it in the initial evaluation bundle.
Medicare Part B covers molecular genetic tests when medically necessary. The neurologist must document the clinical indication with specific ICD-10 codes (e.g., G11.1 hereditary ataxia). Always ask the ordering physician to submit a prior authorization request before the blood is drawn.
Recommended sequence: Movement Disorder Consult → EMG/NCV → Multigene SCA Panel → DNMT1 sequencing (if SCA panel is negative)
Targets the specific gene behind ADCADN — deafness + ataxia + narcolepsy triad. Done only if the standard SCA panel is negative. Same Medicare prior authorization process applies.
Medicare covers genetic counseling visits (CPT 96040) billed by a licensed genetic counselor or physician. Medicare pays 80%; Medigap pays the 20%. Penn Ataxia Clinic has an on-site CGC (Rachel A. Paul, MS CGC). Hopkins also has genetic counselors embedded in the ataxia team.
Before scheduling: confirm "Do you accept Original Medicare?" (not Medicare Advantage). The answer at Hopkins, Penn, and Jefferson is yes.

Places where many of the plants in this app grow wild or are cultivated. Short walks, flat terrain, coastal light.
Sussex CountySeasonal. Most stands open May–October; some run year-round with roots and storage crops. The Route 1 corridor and inland roads through Lewes, Milton, and Millsboro have the highest concentration.




100 sources indexed in NotebookLM, June 2026. Key direct quotes below — expand a section to read.
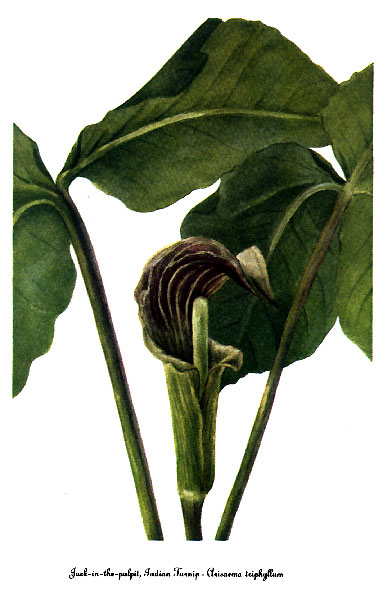

All illustrations are public domain — pre-1928 publications or U.S. government works. Plants are native or naturalized to Delaware and the mid-Atlantic coast, chosen for the coastal wetland, forest edge, and sandy soil habitats of Sussex County.
Notes and highlights are saved to this device only. Email them to yourself for a backup.
Tap the + Save button inside any section to clip it here.
Select any text in the other tabs — a Highlight button will appear.
Add events in any order — dates you remember, approximate or exact. This stays on your device. You decide what, if anything, gets shared with the research tools.
Stored only on this device. Triple-tap the title to reopen.
